Skincare
Mitral Valve Prolapse (MVP): Symptoms, Causes, Diagnosis, and Treatment
Jun
“`
Mitral valve prolapse, often shortened to MVP, sounds like something a dramatic heart valve does when it wants attention. In reality, it is a common heart valve condition in which one or both flaps of the mitral valve bulge backward into the heart’s upper-left chamber during a heartbeat. Sometimes this causes no trouble at all. Other times, it can allow blood to leak backward, a problem called mitral regurgitation.
The good news: many people with mitral valve prolapse live normal, active lives and never need treatment beyond routine checkups. The important part is knowing what MVP means, what symptoms deserve attention, how doctors diagnose it, and when treatment becomes necessary. Think of this guide as a friendly map through the heart’s plumbing systemminus the scary hospital-drama soundtrack.
What Is Mitral Valve Prolapse?
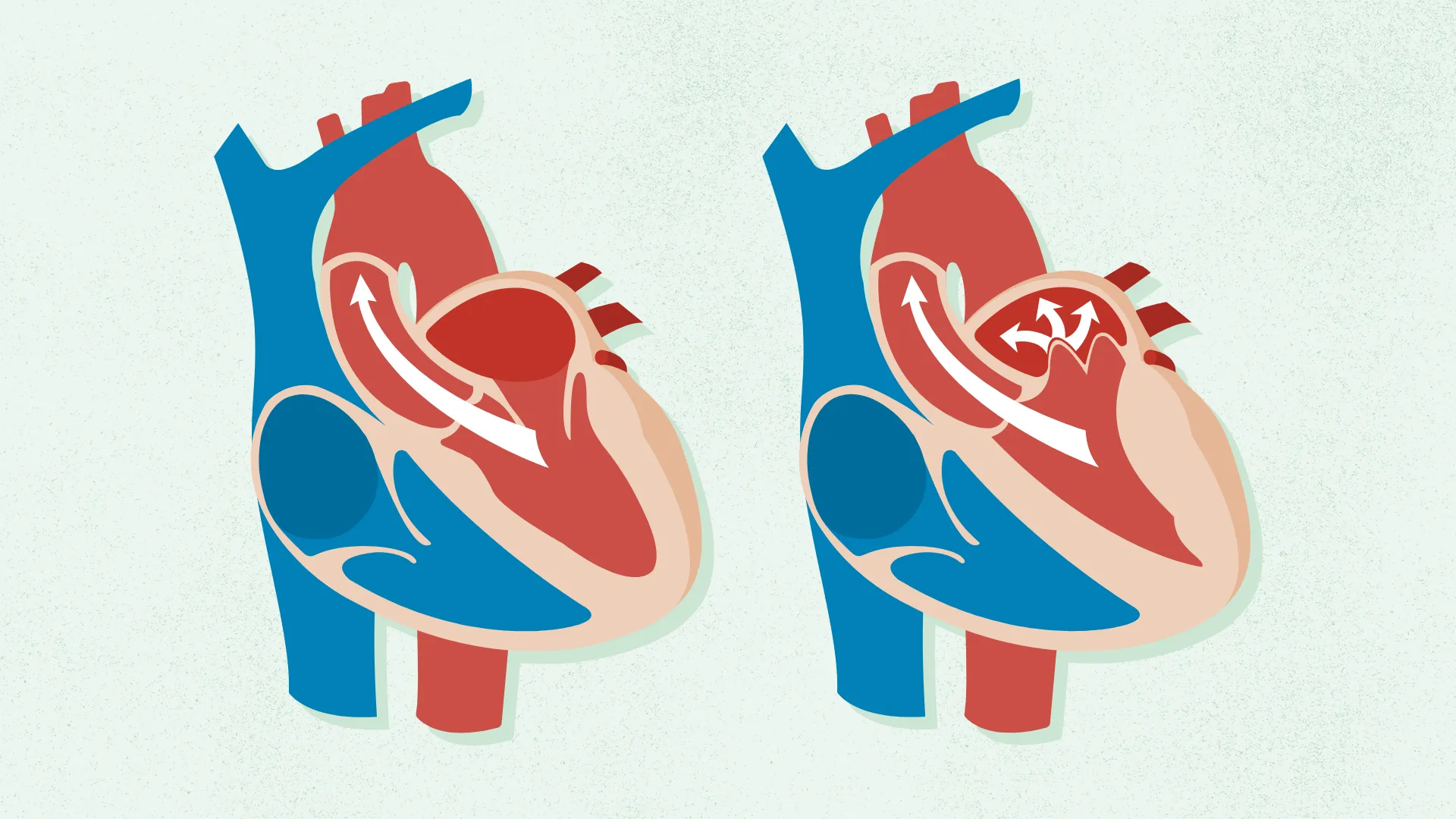
The mitral valve sits between the left atrium and the left ventricle, the two chambers on the left side of the heart. Its job is simple but vital: open to let oxygen-rich blood flow into the main pumping chamber, then close tightly so blood does not travel backward.
In mitral valve prolapse, the valve leaflets are unusually floppy, thickened, stretchy, or shaped in a way that lets them billow back into the left atrium when the heart contracts. This backward movement is the “prolapse.” If the valve still seals well, MVP may be harmless. If the valve does not close tightly, blood may leak backward, creating mitral regurgitation.
MVP has also been called Barlow syndrome, floppy valve syndrome, billowing mitral valve syndrome, and click-murmur syndrome. That last name comes from the sound a clinician may hear through a stethoscope: a click, sometimes followed by a murmur.
How Common and Serious Is MVP?
Mitral valve prolapse is one of the better-known valve conditions, but it is often less dramatic than people fear. Many cases are mild, discovered during a routine exam, and never cause major complications. In these situations, the heart keeps working like a dependable delivery driver who occasionally takes a weird turn but still gets the package there.
The seriousness depends mainly on whether MVP causes significant mitral regurgitation, abnormal heart rhythms, heart enlargement, or symptoms that affect daily life. Mild MVP may only need monitoring. Severe regurgitation may require medications, closer follow-up, or a procedure to repair or replace the valve.
Mitral Valve Prolapse Symptoms
Many people with MVP have no symptoms. When symptoms do appear, they can vary from mild annoyances to signs that the valve is leaking enough to strain the heart.
Common MVP Symptoms
- Heart palpitations, fluttering, skipped beats, or a racing heartbeat
- Chest discomfort that may feel sharp, vague, or unusual
- Shortness of breath, especially during activity or when lying flat
- Fatigue or reduced exercise tolerance
- Dizziness or lightheadedness
- Anxiety-like sensations or awareness of heartbeat
- Cough, especially if mitral regurgitation becomes more significant
- Migraine headaches in some people
Chest pain related to MVP is often not the same as classic coronary artery disease pain. It may happen at rest, feel brief or unpredictable, and not always follow the “worse with exertion, better with rest” pattern. Still, chest pain should never be casually dismissed. The heart does not appreciate being ignored, and it has no customer service department.
Symptoms That May Suggest Mitral Regurgitation
If MVP leads to worsening leakage, symptoms may become more noticeable. Watch for shortness of breath during normal activities, swelling in the ankles or feet, waking up breathless at night, persistent fatigue, or a new irregular heartbeat. These symptoms can suggest that the heart is working harder than it should.
When to Seek Urgent Medical Care
Get urgent help if you experience severe chest pain, fainting, sudden shortness of breath, coughing up pink or frothy mucus, symptoms of stroke, or a fast irregular heartbeat with weakness or dizziness. These symptoms do not automatically mean MVP is the cause, but they do mean the situation deserves immediate medical attention.
What Causes Mitral Valve Prolapse?
MVP often develops because the mitral valve tissue is more elastic or redundant than usual. The valve leaflets may be enlarged, thickened, or supported by chordae tendineaetiny cord-like structuresthat are too stretchy. Imagine a door with flexible hinges: it may close, but it can wobble backward instead of shutting with a clean click.
Possible Causes and Risk Factors
- Genetics: MVP can run in families, and some people inherit valve tissue traits that increase risk.
- Connective tissue conditions: Disorders that affect connective tissue may make valve structures more flexible.
- Myxomatous degeneration: This describes weakening or thickening changes in valve tissue that can make the valve floppy.
- Age-related valve changes: Some valve problems become more noticeable over time.
- Other heart conditions: Conditions that affect the heart’s size, shape, or pumping function can influence valve performance.
Most people did not “cause” their MVP through poor habits. It is not usually the result of eating one too many salty fries or skipping a week at the gym. Lifestyle matters for overall heart health, but MVP itself often reflects valve structure more than personal behavior.
How MVP Is Diagnosed
Diagnosis usually begins with a physical exam. A healthcare provider may hear a click, a murmur, or both while listening to the heart. Because sound alone cannot show the valve clearly, doctors often use imaging tests to confirm the diagnosis and measure whether blood is leaking backward.
Echocardiogram
An echocardiogram is the main test for mitral valve prolapse. It uses sound waves to create moving images of the heart. This test can show how the valve leaflets move, whether the valve leaks, how severe the leakage is, and whether the heart chambers are enlarged.
Electrocardiogram
An electrocardiogram, or ECG/EKG, records the heart’s electrical activity. It may help detect irregular rhythms, skipped beats, or other electrical changes. It does not show the valve directly, but it can provide useful clues.
Holter Monitor or Event Monitor
If palpitations come and go like a mysterious phone notification, a short office ECG may miss them. A Holter monitor or event monitor records heart rhythm over a longer period, helping doctors connect symptoms with actual rhythm changes.
Stress Testing
A stress test may be used if symptoms occur with exercise or if the clinician wants to see how the heart responds to activity. It can help separate valve-related symptoms from other causes of chest discomfort or shortness of breath.
Cardiac MRI, CT, or Catheterization
Advanced imaging may be used when echocardiogram results are unclear or when planning treatment. Cardiac catheterization is not usually needed just to diagnose MVP, but it may be used in selected cases, especially before surgery or when coronary artery disease must be evaluated.
Treatment for Mitral Valve Prolapse
Treatment depends on symptoms, the severity of mitral regurgitation, heart rhythm findings, and whether the heart has enlarged or weakened. For many people, treatment is refreshingly boring: no major intervention, just periodic monitoring.
1. Watchful Waiting and Regular Checkups
If MVP is mild and there is little or no regurgitation, your doctor may recommend routine follow-up. This may include repeat echocardiograms at intervals based on your condition. The goal is to catch changes early, not to turn your calendar into a cardiology-themed escape room.
2. Medications for Symptoms
Medicines do not usually “fix” the prolapsing valve itself, but they may help manage symptoms or complications. Depending on the situation, doctors may consider beta-blockers for palpitations or fast heartbeats, medicines for heart rhythm problems, diuretics for fluid buildup, or blood thinners if atrial fibrillation develops and stroke risk is elevated.
3. Lifestyle and Heart-Healthy Habits
People with MVP are often encouraged to follow general heart-healthy habits: regular physical activity approved by a clinician, good sleep, stress management, not smoking, blood pressure control, and a balanced diet rich in vegetables, fruits, whole grains, lean proteins, and healthy fats.
Some people notice palpitations after caffeine, dehydration, poor sleep, or high stress. Keeping a symptom diary can help identify triggers. It is less glamorous than a detective movie, but sometimes the culprit really is three iced coffees and four hours of sleep.
4. Mitral Valve Repair
If MVP causes severe mitral regurgitation, valve repair is often preferred when it is technically possible. Repair preserves the person’s own valve and may involve reshaping valve tissue, tightening or replacing supporting cords, or placing a ring to help the valve close properly. Repair can be performed through traditional surgery, minimally invasive approaches, or robotic techniques in selected patients and specialized centers.
5. Mitral Valve Replacement
If repair is not possible, the valve may be replaced with a mechanical valve or a biological tissue valve. Mechanical valves can last a long time but usually require lifelong anticoagulation. Biological valves may not require the same long-term anticoagulation in every case, but they can wear out over time. The best choice depends on age, anatomy, health history, personal preferences, and the surgeon’s assessment.
6. Transcatheter Options
For some people who are not good candidates for open surgery, less invasive transcatheter procedures may be considered for mitral regurgitation. One approach is transcatheter edge-to-edge repair, in which a device helps the valve leaflets close more effectively. Not everyone qualifies, but these options have expanded treatment possibilities for selected patients.
Possible Complications of MVP
Most MVP cases remain stable, but complications can happen. The most important is mitral regurgitation, especially if it becomes severe. Over time, significant regurgitation can enlarge the left atrium or left ventricle and may contribute to heart failure symptoms.
Other possible complications include atrial fibrillation, other abnormal heart rhythms, and rarely infective endocarditis, an infection involving the heart lining or valves. Sudden serious rhythm problems have been described in a small subset of patients, but this is uncommon. The practical takeaway is not to panic; it is to follow up appropriately.
Living With Mitral Valve Prolapse
Living with MVP usually means learning your specific risk level. Two people can both have “MVP” on paper and have very different realities. One may need only reassurance after an echocardiogram. Another may need regular imaging, rhythm monitoring, medication, or referral to a valve specialist.
Ask your clinician clear questions: How much regurgitation do I have? Is my heart size normal? How often do I need an echocardiogram? Are my palpitations harmless or do they need monitoring? Are there activity restrictions? Should I see a cardiologist or valve specialist?
For most people, exercise is encouraged rather than feared. However, people with severe regurgitation, fainting, significant arrhythmias, or heart enlargement may need individualized guidance. The best exercise plan is one that supports the heart without pretending every person is training for an Olympic rowing final by Tuesday.
Practical Experience: What MVP Can Feel Like in Real Life
People often describe the experience of mitral valve prolapse as confusing before it is diagnosed. One day the heart feels calm; another day it flutters during a meeting, after coffee, or while lying in bed. That unpredictability can make MVP feel bigger than it is. The first practical lesson is that symptoms and danger are not the same thing. Palpitations can be frightening, but many are benign. Still, they are worth discussing, especially if they are new, frequent, or paired with dizziness or fainting.
A common real-life scenario starts with a routine physical. The provider hears a click or murmur and orders an echocardiogram. The patient then does what modern humans do best: searches the internet, reads three terrifying pages, and mentally updates their will before lunch. A calmer approach is better. The echocardiogram usually provides the key information: whether MVP is present, whether regurgitation exists, and whether the heart is handling it well.
Another experience many patients report is learning the difference between “I have a valve condition” and “I am fragile.” Mild MVP does not automatically mean a person must avoid exercise, travel, work, school, or normal activities. In fact, staying active and maintaining cardiovascular fitness often supports overall health. The smarter move is to ask for personalized guidance rather than self-prescribing a lifetime membership in the Bubble Wrap Club.
Symptom tracking can be surprisingly helpful. A simple log noting sleep, caffeine, stress, hydration, exercise, palpitations, chest discomfort, and shortness of breath may reveal patterns. Maybe palpitations cluster after energy drinks. Maybe they appear during exam stress or after poor sleep. Maybe they occur randomly and need rhythm monitoring. A diary gives your clinician better clues than “my heart did the weird thing again.”
For people with moderate or severe mitral regurgitation, the experience becomes more structured. Follow-up appointments and repeat imaging matter. Some patients feel well even when the valve leak is significant, which is why doctors may monitor heart chamber size and function before symptoms become dramatic. In valve disease, waiting for a crisis is not a strategy; it is more like ignoring a smoke alarm because the furniture is not on fire yet.
Patients who need surgery often discover that “mitral valve surgery” is not one single thing. Repair may be possible and is often preferred when anatomy allows. Replacement may be better in other cases. Minimally invasive and robotic approaches may be options for selected patients, but the best procedure depends on valve anatomy, severity, surgical risk, and the experience of the treatment center. A second opinion at a dedicated valve center can be reasonable when severe regurgitation is diagnosed.
Emotionally, MVP can create a strange mix of relief and worry. Relief because many cases are manageable. Worry because the heart is involved, and the heart is not exactly a casual organ. The best long-term mindset is informed but not obsessed. Keep appointments, understand your test results, follow treatment recommendations, and treat urgent symptoms seriously. Then get back to living your lifepreferably with fewer panic-search spirals and maybe one less giant coffee.
Conclusion
Mitral valve prolapse is a common heart valve condition that ranges from harmless to medically important, depending mainly on whether it causes significant mitral regurgitation or rhythm problems. Many people have no symptoms and need only routine monitoring. Others may experience palpitations, chest discomfort, shortness of breath, fatigue, dizziness, or reduced exercise tolerance.
The most useful test is usually an echocardiogram, which shows how the valve moves and whether blood leaks backward. Treatment may include observation, symptom-focused medications, rhythm management, orin more severe casesmitral valve repair or replacement. With the right follow-up, most people with MVP can understand their risk, protect their heart, and avoid letting a floppy valve run the whole show.
“`
