Beauty Tools & Accessories
Pleural Metastasis in Breast Cancer Recurrence: What to Know
Jun
Note: This article is for general education and should not replace medical advice. Anyone with new or worsening shortness of breath, chest pain, fainting, blue lips, confusion, or rapid breathing should seek urgent medical care.
Breast cancer recurrence has a way of arriving with vocabulary that sounds as if it escaped from a medical spelling bee. “Pleural metastasis” is one of those terms. It is serious, yes, but it is also understandable once we translate it from doctor-speak into human-speak: breast cancer cells have spread to the pleura, the thin lining around the lungs and inside the chest wall. When that lining becomes involved, fluid can collect around the lung, making breathing feel like trying to inflate a balloon inside a shoebox.
Pleural metastasis in breast cancer recurrence is usually considered a form of metastatic breast cancer, also called stage 4 breast cancer. That does not mean there is nothing to do. It means the treatment plan changes from local control alone to a mix of whole-body cancer therapy, symptom relief, careful monitoring, and quality-of-life support. Modern care can include hormone therapy, targeted therapy, chemotherapy, HER2-directed treatment, immunotherapy for selected tumors, drainage procedures, pleural catheters, pleurodesis, and palliative care that focuses on comfort and functionnot giving up, but getting practical.
What Is Pleural Metastasis?
The pleura is a smooth, double-layered membrane. One layer covers the lungs, while the other lines the inside of the chest. Between them is a tiny space with a small amount of lubricating fluid. Normally, this setup lets the lungs glide as you breathe. Very elegant. Very quiet. Very much not something most people think about while unloading groceries.
Pleural metastasis happens when breast cancer cells travel from the original breast tumoror from a previous recurrenceto the pleural lining. These cells can irritate the pleura, block normal drainage pathways, and trigger fluid buildup. When cancer cells are found in the pleural fluid or pleural tissue, doctors may call it a malignant pleural effusion. Not every pleural effusion in someone with breast cancer is malignant, though. Fluid can also come from infection, heart failure, blood clots, inflammation, kidney or liver disease, or even treatment effects. That is why testing matters.
Why Breast Cancer Can Come Back in the Pleura
Breast cancer can recur locally near the breast or chest wall, regionally in nearby lymph nodes, or distantly in organs and tissues such as bones, liver, lungs, brain, or pleura. Cancer cells may spread through the bloodstream or lymphatic system, then settle in a new location where conditions allow them to grow. Some cells can remain quiet for years before becoming active again, which is one reason follow-up care matters even long after initial treatment.
The risk of recurrence depends on many factors: original tumor stage, lymph node involvement, tumor grade, hormone receptor status, HER2 status, genomic test results, response to treatment, and whether recommended therapies were completed. Pleural metastasis is not caused by coughing too hard, sleeping on one side, eating the “wrong” snack, or having a stressful week. Cancer biology is more complicated than that, and blaming the patient is not only inaccurateit is also rude, and cancer is already rude enough.
Common Symptoms of Pleural Metastasis and Malignant Pleural Effusion
Symptoms often come from fluid compressing the lung or from irritation of the pleura. Some people have mild symptoms at first, while others feel a sudden change in breathing. The size of the effusion does not always perfectly match how bad someone feels, because lung health, anemia, anxiety, fitness level, and other cancer sites can all affect symptoms.
Symptoms to Watch For
- Shortness of breath, especially with activity or when lying flat
- Dry cough that does not seem to go away
- Chest tightness, pressure, or pain
- Sharp pain with deep breathing, coughing, or sneezing
- Unusual fatigue or reduced stamina
- Feeling unable to take a full breath
- Rapid breathing or needing extra pillows at night
- Unexplained weight loss, appetite changes, or general decline
Call a healthcare professional promptly if these symptoms are new, worsening, or interfering with normal activities. Seek emergency care for severe shortness of breath, crushing chest pain, coughing blood, fainting, confusion, or symptoms that feel suddenly dangerous.
How Doctors Diagnose Pleural Metastasis
Diagnosis usually starts with a conversation and physical exam. A clinician may listen to the chest and notice reduced breath sounds on one side. Imaging can then show whether fluid is present and how much space it occupies.
Imaging Tests
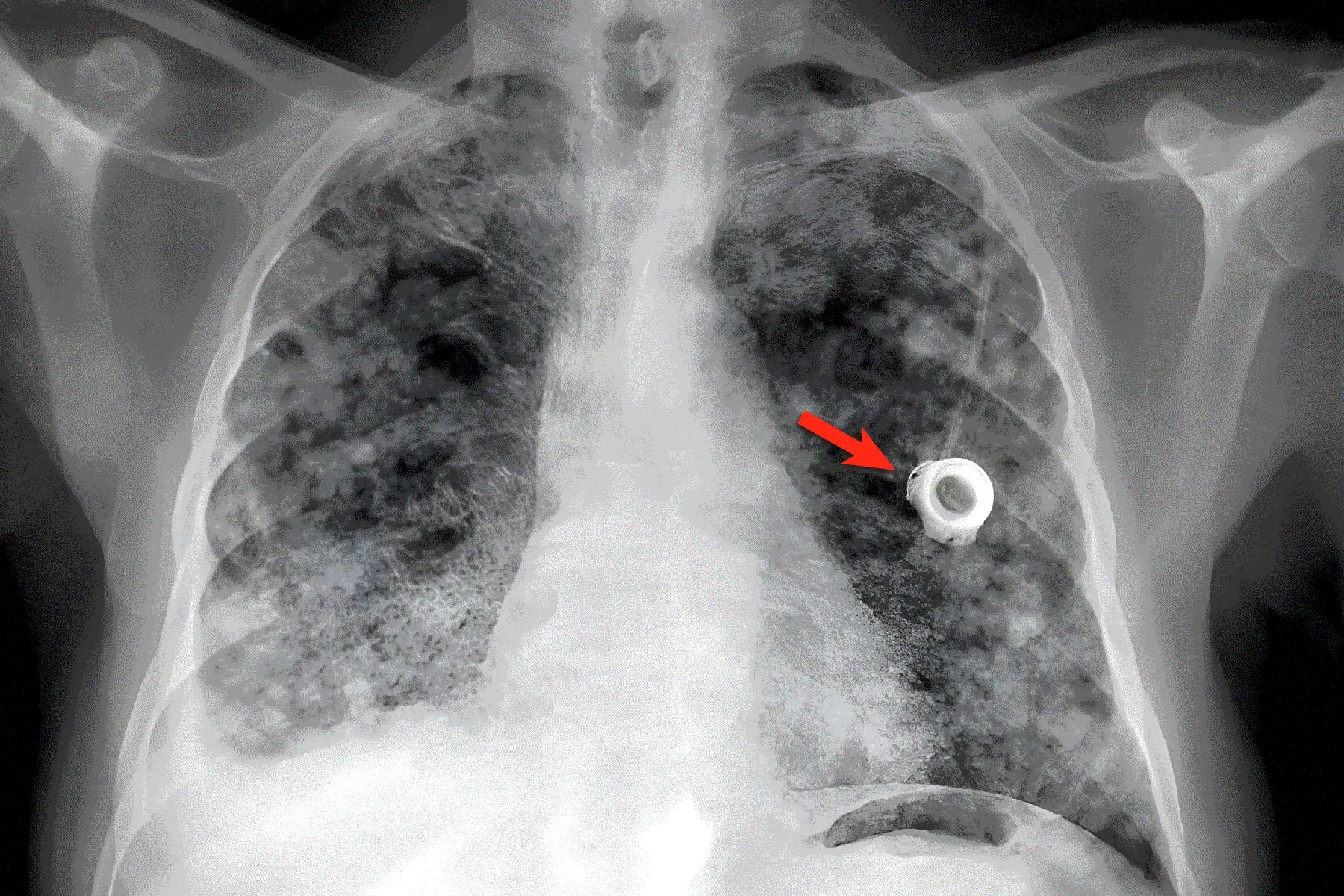
A chest X-ray can often detect moderate or large pleural effusions. Ultrasound helps locate fluid and guide safe drainage. CT scans provide more detail about the pleura, lungs, lymph nodes, chest wall, liver, bones, and other areas. PET/CT may be used in some cases to evaluate active cancer throughout the body, although the best imaging plan depends on the patient’s symptoms and treatment history.
Thoracentesis
Thoracentesis is a common procedure used to remove fluid from the pleural space. A clinician numbs the skin, places a needle or small catheter between the ribs, and drains fluid. The fluid can be tested for cancer cells, infection, protein levels, blood cells, chemistry markers, and other clues. Thoracentesis can also relieve breathing symptoms, sometimes dramatically. Patients may describe it as finally getting “room” to breathe again.
Pleural Fluid Cytology and Biopsy
If cancer cells are found in pleural fluid, the diagnosis becomes clearer. If the fluid test is negative but suspicion remains high, doctors may recommend repeat testing, pleural biopsy, or thoracoscopy, a procedure that allows direct inspection of the pleural space. A biopsy can also help confirm whether the cancer is still breast cancer and whether its receptor status has changed.
Why Rechecking Tumor Biology Matters
Metastatic breast cancer is treated based on biology, not just location. That means doctors often want to know whether the recurrent cancer is estrogen receptor-positive, progesterone receptor-positive, HER2-positive, triple-negative, or carrying certain genetic or molecular changes. Tumors can evolve over time. A cancer that was HER2-negative years ago may test differently later, and hormone receptor levels can shift as well.
This information can shape treatment. Hormone receptor-positive disease may respond to endocrine therapy with targeted medicines such as CDK4/6 inhibitors or other pathway-directed drugs. HER2-positive disease may be treated with HER2-directed therapies. Triple-negative breast cancer may involve chemotherapy, immunotherapy if specific markers are present, antibody-drug conjugates, or clinical trials. For people with inherited BRCA mutations, PARP inhibitors may be considered. The exact plan belongs to the oncology team, but the key idea is simple: identify the cancer’s “settings” before choosing the tools.
Treatment Goals: Control the Cancer and Help Breathing
Pleural metastasis treatment usually has two tracks. The first track treats the cancer throughout the body. The second track manages the pleural fluid and breathing symptoms. A good plan does both. Treating only the fluid without addressing the cancer may lead to repeated procedures. Treating only the cancer while someone struggles to breathe is also not ideal. Breathing is not a luxury feature.
Systemic Therapy
Systemic therapy travels through the body to treat cancer wherever it is active. Options may include endocrine therapy, targeted therapy, chemotherapy, HER2-directed therapy, immunotherapy for selected cases, antibody-drug conjugates, or clinical trial treatments. The choice depends on tumor subtype, prior treatments, side effects, organ function, pace of disease, symptoms, and patient preferences.
If pleural symptoms are mild and cancer therapy is expected to work quickly, doctors may monitor the fluid while starting systemic treatment. If breathing is significantly affected, fluid drainage may be needed right away, even before the longer-term cancer therapy has time to help.
Thoracentesis for Symptom Relief
Thoracentesis can provide fast relief by removing fluid. It is especially useful when doctors need a diagnosis or when the effusion is causing shortness of breath. However, malignant pleural effusions often come back. Repeating thoracentesis may be reasonable for some people, but frequent fluid buildup can turn life into a loop of appointments, needles, and waiting rooms. At that point, longer-lasting options may be discussed.
Indwelling Pleural Catheter
An indwelling pleural catheter is a small tube placed into the pleural space and left in place so fluid can be drained at home. A nurse, caregiver, or trained patient may drain fluid on a schedule using special bottles. This can reduce hospital visits and give people more control over breathlessness. It can be particularly helpful when fluid returns quickly or when the lung does not fully re-expand after drainage.
Pleurodesis
Pleurodesis is a procedure designed to prevent fluid from reaccumulating. A substance, often sterile talc, is introduced into the pleural space to make the pleural layers stick together. If the space closes, fluid has nowhere to collect. Pleurodesis works best when the lung can expand well after drainage. If the lung is trapped by tumor or scarring, a catheter may be more suitable.
Radiation Therapy and Local Treatments
Radiation is not usually the main treatment for widespread pleural metastasis, but it may help with specific painful chest wall lesions, airway compression, or localized symptoms. Surgery is rarely used to remove pleural metastases in breast cancer recurrence, but procedures may be considered for diagnosis, drainage, or complications.
What Pleural Metastasis Means for Prognosis
Pleural metastasis usually means the cancer is advanced, but prognosis varies widely. Some people respond well to treatment for months or years, especially when the tumor biology has effective targeted options. Others may have more aggressive disease or multiple organs involved. Important factors include breast cancer subtype, overall tumor burden, performance status, response to prior treatments, time since original diagnosis, and whether symptoms can be controlled.
It is understandable to search for survival numbers. The internet loves numbers because numbers look confident, even when they are not very personal. Population statistics can describe groups, but they cannot predict one person’s exact path. A better question for the oncology team may be: “What are we trying next, how will we know if it is working, and what symptoms should make us call immediately?”
Questions to Ask the Care Team
- Is the pleural fluid confirmed to be malignant?
- Were receptor tests repeated on the metastatic cancer?
- Is this effusion small, moderate, or large?
- Do you think my shortness of breath is from fluid, cancer, anemia, infection, blood clot, treatment side effects, or more than one cause?
- Should I have thoracentesis now, or can we monitor it?
- If the fluid comes back, would a pleural catheter or pleurodesis fit my situation?
- What systemic treatment is recommended for my subtype?
- How soon will we scan or reassess?
- Which symptoms should send me to the emergency room?
- Can palliative care help with breathing, cough, pain, sleep, anxiety, or planning?
Living With Pleural Metastasis: Practical Comfort Tips
Medical treatment is the foundation, but daily adjustments can make life easier. People with pleural effusion often feel better sleeping with the head of the bed raised or using extra pillows. Small, frequent activities may be easier than one big effort. A shower chair can help conserve energy. Keeping frequently used items at waist height reduces bending and breathlessness. This is not “being lazy”; it is smart energy budgeting.
Breathing techniques may help during moments of mild shortness of breath. Pursed-lip breathingslowly inhaling through the nose and exhaling through gently puckered lipscan reduce panic and improve airflow for some people. A fan pointed toward the face may ease the sensation of breathlessness. However, these tips are not substitutes for medical evaluation, especially when symptoms are new or worsening.
Nutrition can also be tricky. Breathlessness may make large meals uncomfortable, so smaller meals may feel better. Hydration matters, but fluid advice should be individualized, especially if heart, kidney, or liver issues are present. Patients should ask before using supplements because some can interfere with cancer treatments. “Natural” does not always mean harmless; poison ivy is natural, and nobody invites it to dinner.
The Emotional Side: When Breathing Becomes a Full-Time Job
Pleural metastasis can be emotionally exhausting. Shortness of breath is frightening because breathing is supposed to be automatic. When every staircase feels like a negotiation, anxiety can rise quickly. Many people also feel frustrated because they may look “fine” while feeling anything but fine. That mismatch can make it harder for friends, coworkers, and even family to understand.
Supportive care, counseling, oncology social work, pulmonary rehabilitation guidance, support groups, and palliative care can help. Palliative care is not the same as hospice. It can be used alongside cancer treatment at any stage of serious illness to manage symptoms, support decision-making, and improve quality of life. Think of it as an extra layer of helpnot a white flag.
Experiences and Real-Life Lessons From Pleural Metastasis Care
People facing pleural metastasis in breast cancer recurrence often describe the beginning as confusing. One week, they may notice they are winded walking to the mailbox. The next week, climbing stairs feels like a competitive sport nobody trained for. Because fatigue is common during and after breast cancer treatment, many patients first assume they are simply out of shape, stressed, or still recovering. That is understandable. The body does not send push notifications labeled “pleural effusion detected.” It sends vague clues, and doctors help decode them.
One common experience is relief after the first thoracentesis. A patient may arrive short of breath, anxious, and unsure what is happening. After fluid is drained, breathing may improve quickly. Some describe it as “getting half my lung back.” Others feel only partial relief, which can happen if there are other causes of breathlessness, such as anemia, lung inflammation, blood clots, infection, or cancer spread in other areas. This is why follow-up after drainage is important. The procedure is not only treatment; it is also a diagnostic clue.
Another frequent lesson is that recurrent fluid requires planning, not panic. If the effusion returns, patients may feel discouraged: “Didn’t we just drain this?” Unfortunately, malignant pleural effusions can behave like an unwanted subscription service. They may keep renewing unless the underlying cancer responds or the pleural space is managed with a longer-term approach. Indwelling pleural catheters can be life-changing for some people because they allow regular drainage at home. The idea of having a tube can sound scary at first, but many patients adjust quickly once they realize it may reduce emergency visits and help them breathe more comfortably.
Patients also learn the value of tracking symptoms. A simple notebook or phone note can record breathlessness level, cough, chest pain, oxygen readings if recommended, drainage amounts, fever, medication changes, and activity tolerance. Patterns help the care team make decisions. For example, draining large amounts frequently may support the need for pleurodesis or a catheter. New fever after a catheter is placed may require quick evaluation for infection. Sudden severe shortness of breath may point to something more urgent than routine fluid buildup.
Family communication matters too. Loved ones may want to help but not know how. Specific requests work better than general ones. “Please drive me to Thursday’s scan,” “Please carry the laundry,” or “Please sit with me during the oncology call and take notes” is easier to answer than “Please understand everything I’m feeling,” which is a very large assignment with no instruction manual. Cancer caregiving is a team project, and like all team projects, it improves when someone writes things down.
Many patients say their best care experiences happen when oncology, pulmonology, interventional radiology, nursing, and palliative care communicate clearly. Pleural metastasis sits at the intersection of cancer control and breathing mechanics. That means a medical oncologist may focus on systemic therapy, while a pulmonologist or interventional specialist helps manage the fluid. When the team works together, patients are less likely to feel bounced around like a medical ping-pong ball.
Finally, people living with pleural metastasis often discover that hope changes shape. Hope may mean a good scan. It may mean walking around the block. It may mean sleeping through the night without coughing. It may mean choosing a treatment that protects quality of life. None of these hopes are small. In advanced breast cancer care, success is not only measured in lab values and imaging reports; it is also measured in breath, comfort, time, clarity, and moments that still feel like life.
Conclusion
Pleural metastasis in breast cancer recurrence means breast cancer has involved the pleural lining around the lungs. It may cause malignant pleural effusion, leading to shortness of breath, cough, chest discomfort, fatigue, and reduced activity tolerance. Diagnosis usually involves imaging and fluid testing through thoracentesis, sometimes followed by biopsy. Treatment may include systemic breast cancer therapy plus procedures such as thoracentesis, indwelling pleural catheter placement, or pleurodesis to control fluid and improve breathing.
The most important message is this: pleural metastasis is serious, but it is not a reason to stop asking good questions or seeking symptom relief. Breathing comfort matters. Tumor biology matters. Quality of life matters. A strong care plan should explain what is happening, what can be treated, what symptoms require urgent help, and how the patient can live as fully as possible while treatment continues.
